Disclaimer: The author of the content below is not a medical professional and does not have any medical training. As such, the contents on this page, including text, graphics, images, and any other material are for informational purposes only. The Content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Our full medical disclaimer can be found by clicking here.
VEEG
On Monday morning we went to the hospital for James’ overnight VEEG. The last time we did a VEEG was a year and a half ago, in October of 2010. That one was done at home. This time, being in the hospital, it was a little different. They gave us a private room in the PICU (pediatric intensive care unit). I don’t really know why they decided to put us in the PICU; James wasn’t in critical condition. Maybe they just wanted us to be as comfortable as possible, and the PICU has some nice sized rooms.
After we got settled into the room, it was time to get James all wired up with all of the electrodes. Here are a couple of pics of the tech putting the electrodes on his head.


After all of the electrodes were attached to his head, she wrapped his head in gauze to keep everything in place.

The electrodes are attached to a computer which also has a camera attached to it so they can see if James has any visible reactions during a seizure. There is also a button that we push when we see him having a seizure. Pushing the button puts a mark on the chart so that when the neurologist is reviewing it, he knows which areas to look at. It’s interesting that they don’t actually watch and monitor the VEEG at the hospital we were at. Instead, the feed is sent to another hospital 30 miles away. There was somebody on that end watching James all night long. It was a little bit creepy knowing that someone was watching us. We had to make a mental note not to pick our noses in view of the camera. Ha ha!
Here is a pic of what an EEG looks like:
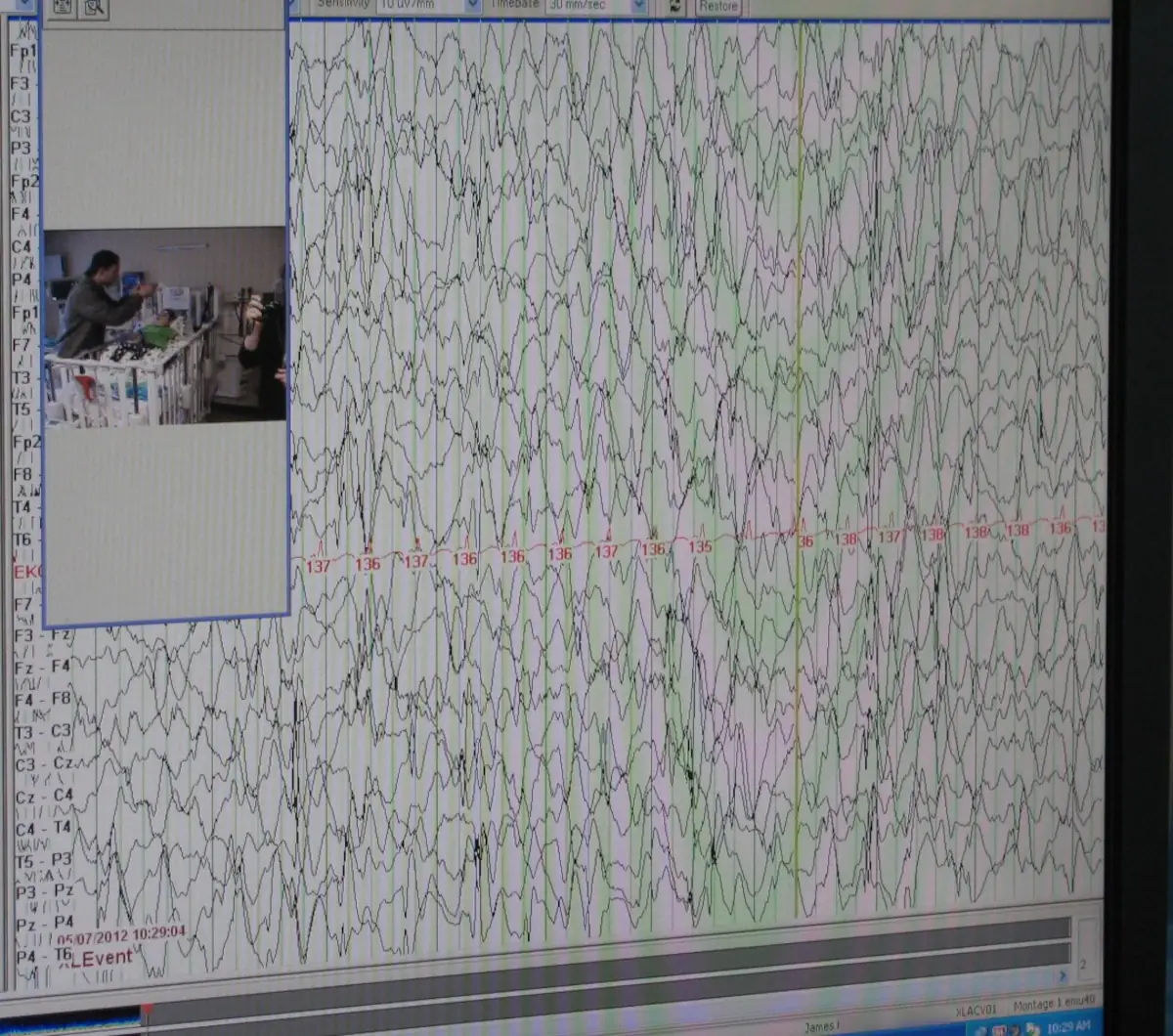
In the first few hours after he was hooked up, they were able to see four seizures, both through the electrodes, and visibly on the camera. We thought this was a good thing, because that is why we were there. Then they started to see a lot of seizure activity through the electrodes, but they weren’t visible through the camera. He was having seizures that we could not visually see. The neurologist was a bit worried and requested that an IV be put in just in case they needed to give James a quick dose of an antiseizure med. Shortly after the IV was in, they thought that James was “in status”. What is that? Status epilepticus is a seizure that lasts longer than five minutes or having more than one seizure within a five-minute period, without returning to a normal level of consciousness between episodes. This is considered a medical emergency, so they used the IV and gave James some phenobarbital.
After getting the phenobarbital, James’ brain really calmed down. It was like a night and day difference. It pretty much knocked him out. He fell asleep at about 4 pm (about an hour after the phenobarbital) and was still sleeping at 8:30 am Tuesday morning.
The neurologist stopped into the room early Tuesday afternoon to give us his assessment. The good news is that James was not “in status” like they thought he was. There was just a lot of seizure activity. He wasn’t 100% sure, but it looks like the seizures were coming from the right front of the brain. He would like James to have an MRI and a MEG scan, which should be able to pinpoint where the seizures are coming from. The doc made another change to James’ seizure meds—increased the dose on one and decreased the dose on another—and said that we were free to go home.
Nursing Care
Somebody had mentioned to Stacy a while back that we should talk to our insurance company to see if James is eligible for nursing care. Apparently, he is, so Thursday the director of nursing care came over to meet us and get trained on James. She came back on Friday to take care of James while Stacy went out to get a haircut. We only have a certain amount of nursing hours that we can use. For now, we’re going to try to have a nurse on Thursdays and Fridays from 8 am to 2 pm, and then we will reassess in about 30 days. It will be a bit strange to have someone else in the house taking care of James, but I think it will be good for Stacy to be able to get out for a bit and have a little break from James during the week.



{kind=link}